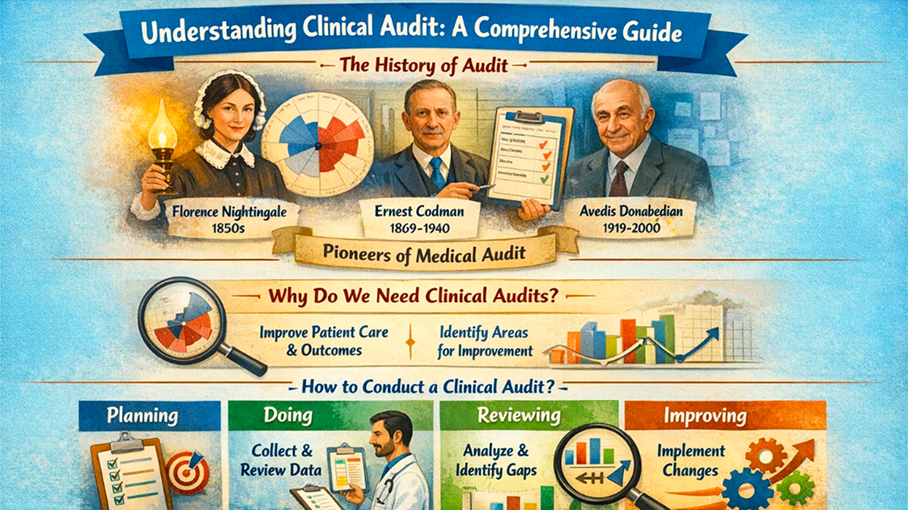
A clinical audit is not a new concept in the field of medicine. The history of audit dates to the time of Florence Nightingale, popularly known as "The lady with the lamp". She was one of the first to use medical statistics to understand the nature of infections in hospitals and battlefields. But her contribution didn't stop there. She used pictorial representation of data to convince politicians to implement necessary changes, which underlines the importance of effective communication in the process of audit.
Ernest Codman (1869-1940), another stalwart in the field, laid great emphasis on monitoring surgical outcomes. He advocated the idea that every hospital should follow up with every patient it treats to determine whether the treatment has been successful. If not, there should be an inquiry into why the treatment failed, with the aim of preventing similar failures in the future.
Avedis Donabedian (1919-2000), one of the pioneers, defined clinical audit as a quality improvement process that seeks to improve patient care and outcomes through systematic review of care against explicit criteria. However, the audit process does not stop at review. If changes are indicated, they are implemented, and further monitoring is used to confirm improvement in healthcare delivery.
Why Do We Need Clinical Audits?
Clinical audits are pivotal in assessing if a certain aspect of healthcare is meeting a recognized standard. They help us understand where our service is doing well and where improvements could be made. For instance, audits can assess pre-op skin preparation in wards, the timing and duration of prophylactic antibiotics, and the choice of antibiotics for skin and subcutaneous infections, among other things.
How to Conduct a Clinical Audit?
The process of conducting a clinical audit can be broken down into four main steps: Planning, Doing, Reviewing, and Improving.
Planning
The planning phase involves selecting a topic, forming a team, setting aims and objectives, writing the proposal, identifying standards and benchmarks, and creating a data collection tool.
Choosing a topic
If you are new to clinical audit, choose a topic that is a “low hanging fruit” and one that be done with minimal effort. After you have completed a few audits, you can move to a topic that can be of high cost, and volume. Another way is to choose a topic that is of risk to staff or patients or is a regular pain issue for you, your staff, or your patients. Another point to consider is that evidence to decide the standards against which you would compare your current practice should be available.
Forming a team
Establish a diverse team that includes members from different disciplines and levels within the organization. Consider all the required expertise and form a multidisciplinary team. This will provide a well-rounded perspective and ensure that a variety of insights are considered during the audit process. Especially do not leave the frontline workers. Their wisdom goes a long way in making changes that are practical and implementable. Last, the team members should be available and committed.
Setting aims and objectives
The aims and objectives should be clearly defined. The aim is the overall purpose of the project, and objectives are the specific tasks to be undertaken to achieve the aim. These objectives should be SMART: specific, measurable, achievable, relevant, and time bound. They should align with the overall purpose of the audit and help guide the team towards meaningful improvements.
Writing the proposal
Create a proposal outlining the rationale for the audit, the scope of the project, the methods to be used, and the expected outcomes. The proposal should include the background, need for improvement, project overview, aims and objectives, expected outcomes, benefits, and budget. This need not be detailed unless the audit is a complex one. Try to fit it one page. In fact, there is an audit methodology called A3 process where all details and activities of an audit are tracked in one A3 page. This document will serve as a roadmap for the audit and help keep the team focused on the task at hand.
Identifying standards and benchmarks
Research existing standards and benchmarks related to the chosen topic. These will serve as a point of comparison to evaluate current practices and identify areas for improvement. Ensure that the standards are evidence-based and relevant to the context of the audit. If standards are not available, gather a team of experts on that topic and try to get a consensus on the standard that you want to set for your hospital.
Creating a data collection tool
Develop a tool to collect relevant data during the audit process. This could involve surveys, interviews, observations, or reviews of medical records. The tool should be easy to use, reliable, and capable of capturing the information needed to assess performance against the established standards.
Doing the audit
The 'doing' phase involves selecting a sample size, observing current practice, and collecting necessary data. Data collection can be prospective or retrospective and can involve incident reports, patient record reviews, chart audits, analysis of clinical data, direct observation, environmental assessments, process mapping, surveys, questionnaires, interviews, patient surveys, and focus groups.
Selecting the sample size
Selecting the sample size is a crucial step in the audit process. It involves determining the number of participants or data points needed to be representative. Remember an audit is not a research project. Do not fret about factors such as power analysis, confidence intervals, effect size estimation etc. Just use a simple calculation depending on the number of beds available to obtain a sample size.
Observing current practice
This phase allows us to understand how procedures are currently being carried out in real-world settings. By directly observing practices, we can assess compliance with established protocols, and pinpoint any deviations from standard practices.
Collecting data
Observed data is collected using the form designed earlier. The data collected during an audit provides valuable insights that can help identify areas for improvement. During the data collection phase, it is essential to ensure accuracy, consistency, and attention to detail. Much like the familiar “JIJO-Jargon in, jargon out” used in the IT, clean data is necessary for drawing valid conclusions from the audit.
One important point to consider. When you observe, it is very tempting to provide immediate solutions. Unless it compromises safety, do not jump to quick fixes while collecting data. Just collect necessary data during this phase and defer analysis and conclusions to the next phase and improvements to the final phase of the audit.
Reviewing
The reviewing phase is also called the “study” phase. It involves analysing the collected data, and comparing it with standards, to identify areas of improvement. The data can be analysed using again using simple descriptive statistics, frequency distribution and percentage calculation.
QI improvement tools
The commonly used quality improvement tools are the fishbone analysis (Ishikawa diagram) and pareto (80:20) analysis. These tools help in identifying the root causes of any issues discovered during the audit. The fishbone diagram allows for a systematic analysis by categorizing potential causes into different groups, such as people, process, environment, and equipment. On the other hand, the Pareto analysis focuses on the vital few factors that contribute to the majority of problems, enabling us to prioritize our efforts effectively.
Involve the team
During the reviewing phase, it is crucial to involve all stakeholders and relevant teams to ensure a comprehensive understanding of the data and potential improvements. Collaboration and clear communication are key to implementing successful changes based on the audit findings.
Improving
The final phase, 'improving', involves selecting methods for improvement, prioritizing, and sustaining the improvement. Improvement methods can include Plan-Do-Study-Act (PDSA) Cycle, Quality Improvement Teams, Root Cause Analysis (RCA), tracking Performance Metrics and KPIs, and Education and Training.
Prioritizing improvements
At the end of an audit, there are usually quite few improvements that will be begging for your attention. You should take time to consider the most vital or important changes. Consider solutions that benefit the patient, easy and low-cost solutions, practicality. Aim for small wins in each cycle. Remember audits are a continuous process and you should aim for incremental changes. This strategy will serve you and the organisation well in the long term.
Sustaining Improvements
To sustain the improvement, the audit process should be repeated until all changes have been implemented and improvements have been achieved and sustained. The process should be done multiple times and should be of short duration (weeks rather than months) so that changes can be implemented as soon as possible.
In summary, conducting a clinical audit involves planning, doing, reviewing, and improving. Understanding and implementing this process can result in significant improvements in patient care and outcomes.
